

Difference Between Esophagus And Trachea: Function & Conditions
The oesophagus and trachea are tubular structures with distinct roles in the digestive and respiratory systems, respectively. While the oesophagus transports food to the stomach by peristalsis, the trachea conducts air to the lungs with the help of cartilaginous rings. This guide compares their anatomy, layers, functions, and exam-relevant differences for Class and NEET biology.
This Story also Contains
- What Are the Oesophagus and Trachea?
- Anatomy of the Oesophagus
- Anatomy of the Trachea
- Function of the Oesophagus
- Function of the Trachea
- Difference Between Oesophagus and Trachea (Tabular Form)
- Physiological Comparison
- Oesophagus vs Trachea NEET MCQs (With Answers & Explanations)
- Recommended Video for the Difference Between Esophagus and Trachea
What Are the Oesophagus and Trachea?
The oesophagus and trachea are both tubes in the human body and have various roles to play in the human system; the respiratory system and the gastrointestinal system. The oesophagus is a muscular canal, which carries food and liquids from the mouth through the pharynx to the stomach while the trachea or windpipe is a tube that also helps to transport air to and from the lungs. This goes a long way in recognising the relation between biological science since the two structures aid in establishing the elementary framework of intricate mechanisms and diseases.
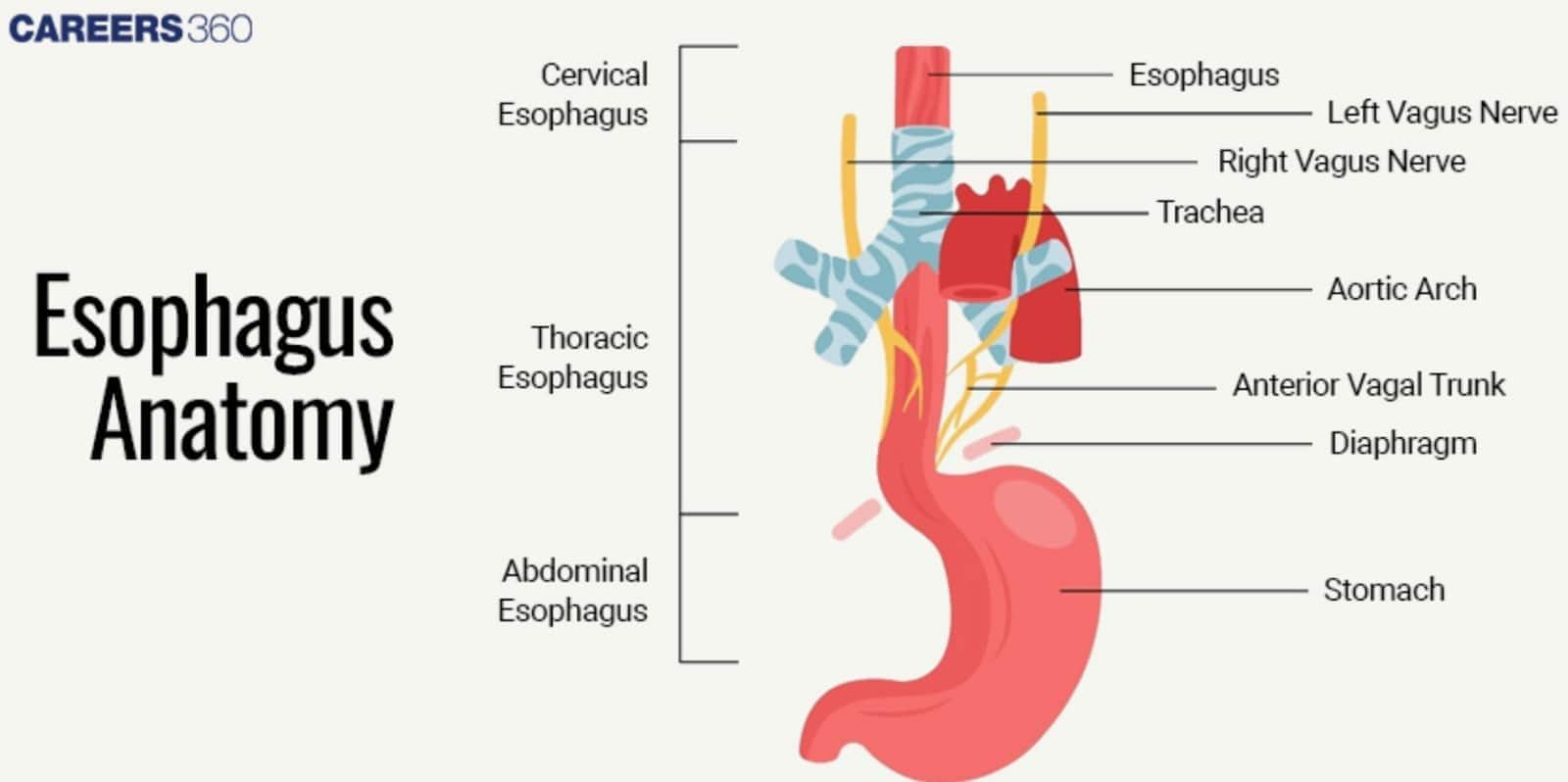
Anatomy of the Oesophagus
Oesophagus is a muscular tube that leads straight from the pharynx, or the throat, to the stomach. It is located dorsally to the trachea but ventral to the spine and extends from the lower end of the pharynx to the upper section of the stomach.
Layers of the Oesophagus
The oesophagus has three layers inherent to the muscle while the fourth and the outermost layer are derived from the skin.
Mucosa: The first layer for protection also has stratified squamous epithelium.
Submucosa: This layer is made of connective, vascular tissue, nerve bundle, and secretion of mucus by glands to facilitate and moisten for easy passage for foods.
Muscularis: Responsible for controlling and moving the food to the stomach. The superior one-third contains only skeletal muscles; the middle one-third contains both skeletal and smooth muscles; and the remaining one-third receives only smooth muscles.
Adventitia: A submucous layer of connective tissue that anchors the oesophagus to neighbouring structures.
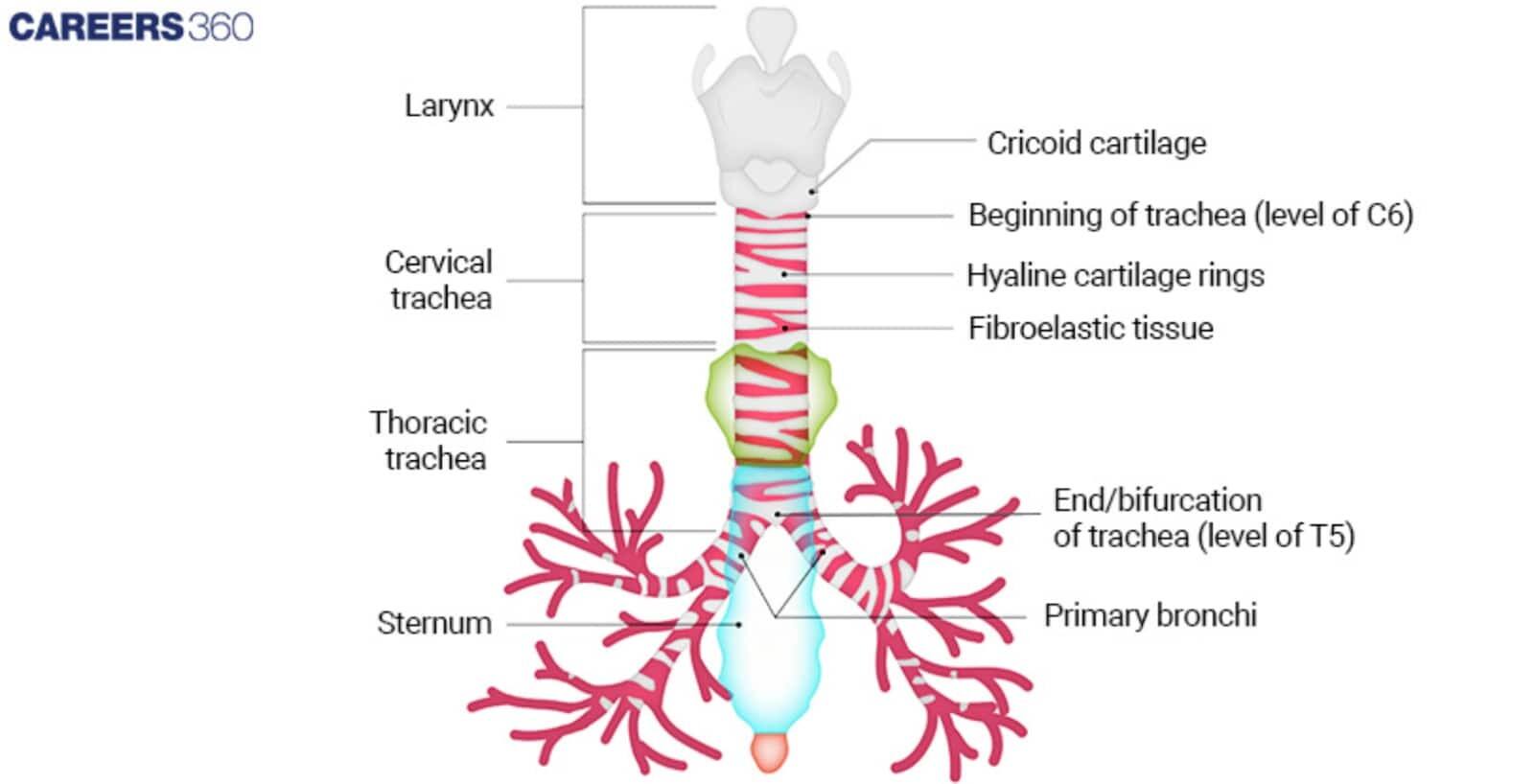
Anatomy of the Trachea
The trachea, also known as the windpipe, is an essential organ in the respiratory system. It is a tube stretching from the larynx to the bronchi, from which it branches into the right and left bronchi. The trachea is situated in front of the oesophagus and formed by the two cartilages in the neck and upper chest.
Structure and Layers
The trachea consists of several layers, each contributing to its function and structure:
Mucosa: Ciliated pseudostratified columnar epithelium. Mucus works to capture dust and other particles; cilia propel the mucus with the dust to the pharynx where it can be swallowed or coughed out.
Submucosa: Comprises connective tissues, blood vessels, nerves and the seromucous glands that provide more mucus required for lubricating and for entrapment.
Hyaline Cartilage: The trachea is connected from anterior to posterior by 16-20 semicircular rings of hyaline cartilage which offer the rigidity and ensure that there is no blockage of the airway.
Adventitia: The last course of connective tissue that gives additional support and binds the trachea to the other connective tissues.
Function of the Oesophagus
The functions of oesophagus includes:
It has the simple role of conveying solids and liquids taken in through the mouth towards the stomach.
This is done by rhythmic contractions of muscles popularly referred to as peristalsis.
The oesophagus also has a muscular ringtone called the upper oesophagal sphincter (UES) and lower oesophagal sphincter (LES) that control the opening and closing of the oesophagus to avoid regurgitation of food.
Function of the Trachea
The functions of trachea includes:
Its major role is thus to act as a conduit through which air can pass from the larynx to the bronchi and then to the lungs.
The trachea has certain functions as a barring element, humidifying, and warming the air before getting into the lungs.
The cilia and the mucus in the lining of the bronchi and the alveoli filter off dust, bacteria and other particles which could harm the lung.
Difference Between Oesophagus and Trachea (Tabular Form)
It is one of the important difference and comparison articles in Biology. The important features are listed below-
| Feature | Esophagus | Trachea |
|---|---|---|
Location in the Body | Posterior to the trachea, extending from the pharynx to the stomach | Anterior to the oesophagus, extending from the larynx to the bronchi |
Tissue Composition |
|
|
Presence of Cartilage | Absent | Present (C-shaped hyaline cartilage rings) |
Length and Diameter | Approximately 25 cm in length; about 2 cm in diameter | Approximately 10-12 cm in length; about 2.5 cm in diameter |
Physiological Comparison
The physiological functions are listed below:
Role in digestion
Prevents backflow of food
Muscle coordination essential
Trachea
Role in respiration
Protects airway from collapse
Filters and humidifies air
Comparing Physiological Functions of the Oesophagus and Trachea
It is one of the important difference and comparison articles in Biology. The important functions are listed below-
| Function | Esophagus | Trachea |
|---|---|---|
Primary Role | Transports food and liquids from the mouth to the stomach | Conducts air from the larynx to the bronchi and lungs |
Peristalsis/Airflow | Peristalsis: Coordinated muscular contractions to move food | Airflow: Continuous airflow for respiration, supported by cartilage |
Airway Protection | Prevents food and liquid from entering the airway | Hyaline cartilage rings prevent airway collapse; mucus traps particles |
Mucosal Function | Mucosa: Protects against abrasion from food | Mucosa: Traps dust and pathogens; cilia move mucus upwards |
Oesophagus vs Trachea NEET MCQs (With Answers & Explanations)
Important questions asked in NEET from this topic are:
Layers of the oesophagus and Trachea
Oesophagus vs Trachea
Practice Questions for NEET
Q1. The outer wall of the esophagus is not lined by the serous membrane. Instead, it contains
Adventitia externa
Lamina propria
Adventitia interna
Muscularis tunica
Correct answer: 1) Adventitia externa
Explanation:
As we have learned in Serosa: It is present only in the region of the alimentary canal within the abdominal cavity. Instead of serosa, the mouth, pharynx, and oesophagus have a dense sheath of collagen fibers called the adventitia. The outer wall of the oesophagus is not lined by a serous membrane, The outer wall is seen in the form of an irregular coat of yellow elastic dense fibrous connective tissue called adventitia externa or tunica adventitia.
Hence, the correct answer is option 1) Adventitia externa.
Q2. Which of the following structures prevents the entry of food particles into the trachea during swallowing?
Glottis
Uvula
Epiglottis
Both a & c
Correct answer: 3) Epiglottis
Explanation:
The Glottis is the opening of the pharynx into the trachea and is always open during the process of respiration. The uvula is a soft muscular structure preventing the entry of food into the nasal cavity during swallowing. The Glottis is covered by a flap-like structure called epiglottis which helps prevent the food particles from moving into the trachea during swallowing instead of the food pipe.
Hence the correct answer is option 3) Epiglottis.
Q3. Heartburn or gastroesophageal reflux disease is caused when
The oesophagus is open during swallowing
Movement of food from the pharynx into the esophagus is altered
The gastro-esophageal sphincter does not completely close
None of the above
Correct answer: 3) The gastro-esophageal sphincter does not completely close
Explanation:
When the gastro esophageal- sphincter does not completely close, the stomach’s contents can reflux (that is, back up into the oesophagus), causing heartburn or gastroesophageal reflux disease (GERD).
Hence, the correct answer is option 3) the gastro-esophageal sphincter does not completely close.
Also Read:
Recommended Video for the Difference Between Esophagus and Trachea
Frequently Asked Questions (FAQs)
Diagnostic procedures for the trachea include:
Bronchoscopy: An examination in which a physician employs a bronchoscope to examine the trachea and bronchi with a closer look at them. One way it assists in the diagnosis includes Obstructions, infections or any abnormality that may also be detected.
Chest X-ray: A technique of taking pictures that can help identify problems with the trachea, including, but not limited to, stricture, expansion, collapse, or any object lodging in it.
CT Scan (Computed Tomography): Enables cross-sectional images of the trachea to be viewed leading to the diagnosis of conditions like tracheal stenosis or tumour.
Pulmonary Function Tests: analyse the workings of the respiratory system, specifically the capability of air to pass through the trachea and bronchi.
The trachea of the respiratory system is mainly to allow free movement of air from the larynx to the bronchi to the lungs. It also filters, humidifies and warms the air breathed in before it gets to the lungs. closure of the trachea and protection of the airway from the particles Since they are C-shaped, these rings do not allow the collapse of the trachea.
In a diagram, the oesophagus and trachea can be differentiated by their structures and surrounding features:
Esophagus: Looks more like a cylindrical tube that has smooth muscles and no cartilage; lies behind the trachea. It normally has a more flexible and collapsible structure, usually about the support mechanism of the building or construction.
Trachea: Out looks like a cylindrical tube that has C-shaped hyaline rings to support its patency or open windpipe. It is situated in front of the esophagus and its mucosal lining as well as its accompanying cartilaginous ring is more well-developed and substantial.
Common diseases affecting the oesophagus include:
Gastroesophageal Reflux Disease (GERD): A condition by which the stomach acid sometimes flows backwards into the oesophagus and brings along with it a burning sensation.
Esophagitis: Irritation of the oesophagus due to some infections, allergies, or substances ingested by the body.
Esophageal Cancer: Cancer that develops in this part of the digestive system thereby interfering with the normal functioning of the esophagus.
Achalasia: A pathology/ disease resulting from the inability of the lower esophageal sphincter to open allowing passage of food into the stomach.
The oesophagus's primary purpose is to channel materials that have been taken through the mouth down to the stomach. In this fashion, several coordinated muscular contractions, called peristalsis, propel the taken materials downwards.
